
Research Article | DOI: https://doi.org/10.31579/2578-8868/163
1* Cognitive Science Intervention Laboratory (LABICC), Department of Psychology (FAPSI), Amazon Federal University (UFAM), Manaus, Brazil.
*Corresponding Author: Raquel Lira de Oliveira Targino, Amazon Federal University, Avenida General Rodrigo Otávio, 3000. Department of Psychology – FAPSI, Bloco X, Mini campus. Cognitive Science Intervention Laboratory – LABICC.
Citation: Raquel Lira de Oliveira Targino, Nazaré Maria de Albuquerque Hayasida (2021) Quality of Life of Drug Users. J. Neuroscience and Neurological Surgery. 8(4); DOI:10.31579/2578-8868/163
Copyright: © 2021 Raquel Lira de Oliveira Targino, This is an open-access article distributed under the terms of The Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited
Received: 26 February 2021 | Accepted: 15 March 2021 | Published: 22 March 2021
Keywords: quality of life; sf-36; drug users; unified health system
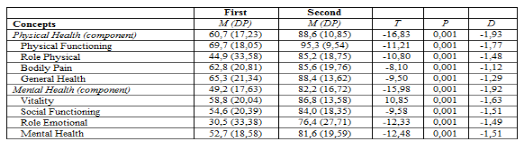
The aim of this study was to analyze the quality of life of drug users hospitalized for treatment through the SF-36. We executed a quantitative-descriptive and cross-sectional research. A total of 52 patients (47 men and 5 women) participated in this study. Our results showed low scores on the physical (M=60), (DP=17,23) and mental (M=49), (DP=17,63) concepts in the first application; however, they showed significant improvements in the second application (M=88.6), (DP=10,85) and (M=82.2), (DP=16,72), respectively. The physical functioning (M=69), (DP=18,05) and vitality (M=58.8), (DP=20,04) concept were highlighted with low initial scores. Nevertheless, significant statistical differences were observed at the end of the treatment: (M=95.3), (DP=9,54) and (M=86.8), (DP=13,58), respectively. We concluded that the therapeutic interventions conducted by the multidisciplinary team from the institution contributed to improving these patients’ quality of life perception, as well as cooperated to increase adherence to treatment.
QoL: Quality of life, SF-36: Item Short-Form Health Survey
Quality of life (QoL) can be understood as the way in which each subject perceives himself within the set of moral and cultural values in which he lives, in relation to his position in the world, to his objectives, goals, expectations, standards and also concerns (Who, 1997). Therefore, it is a broad concept, and it is complexly influenced by the individual's physical health, psychological state, independence level, social relationships, personal beliefs, as well as his or her relationship with the environment. Hence, it is evident that although health care does not alter all factors related to the QoL, such factors may inevitably affect health state and, consequently, the QoL (Who, 1997).
Thus, the QoL concept involves issues related to social relationships, along with other aspects of life, for instance, health, education, work, purchasing power and everything related to well-being and happiness, according to the individual's perception. Therefore, there is a particular difficulty in establishing a single concept, since the perception of the QoL may differ amongst cultures, from time to time, from person to person and even in the same individual it may change over time. In this perspective, the QoL can also be understood as the perception of well-being resulting from a set of personal and socio-environmental parameters that characterize the conditions in which the human being lives. The QoL adds in its scope the representations of disease, prejudices, beliefs, personal convictions, emotions, symptoms, and treatments. Thus, the health-disease binomial is only one of the factors that may interfere in the QoL (Benincasa, 2010; Menezes, 2006; Nahas, 2010 apud Valentim et al., 2014; Seabra et al., 2013).
According to Buss (2000), the QoL affects health and health itself strongly influences the QoL of individuals. It is also a consensus that the determinants and conditionals of the health-disease process that form the individuals’ life are equally important for achieving an adequate state of health. In this sense, the fact of understanding health in a more comprehensive way allows it to be directly related to well-being and QoL and not just as the absence of disease. Hence, it integrates both subjective and multidimensional characteristics, enabling that, in an investigation about QoL, individuals and the perception of themselves and their social context are valued, and not just the presence or not of disease (Seidl e Zannon, 2004).
Studies in the area of QoL have been increasingly frequent, especially in the public health scope, whose focus is to not only reduce the risks of diseases in the population but also to increase the potentialities for health. Therefore, QoL is intrinsically related to health promotion, because it aims to promote and reduce vulnerabilities and health risks related to their determinants and conditionals. Promoting health means overcoming the avoidance of disease and lengthening life to ensure means and situations that amplify the QoL, on a daily basis, thus, increasing the autonomy capacity and the standard of well-being, which are socially defined values and are therefore subject to individual beliefs, values and choices (Brasil, 2006; Buss, 2000; Tran et al., 2020).
The literature points to the grand social and scientific relevance of QoL. Therefore, within the health scope, measuring it is fundamental not only to assess the therapeutic results but also to develop areas with needs for more efficient therapeutic strategies to adjust the therapeutic interventions to the stage of readiness for the change presented by the subject during treatment. It is also worth noting that, currently, QoL has been considered as a possible parameter for evaluating the impact of a certain pathology, as well as for diagnostic and/or therapeutic interventions in the individual’s life, being also used as a remission or relapse predictor (Castro et al., 2007; Menezes, 2006; Pereira et al., 2012; Szupszynski e Oliveira, 2008; Oliveira et al., 2014; Valentin et al., 2014).
Scientific evidences regarding the evaluation of QoL in chronic diseases, for instance, renal disorders, arthritis, arterial hypertension, in addition to substance dependence, demonstrate that chemical dependents have deteriorated QoL compared to the general population (Marini et al., 2013; Menezes, 2006; Vanelli e Freitas, 2011). In general, studies have reported a significant loss of QoL in alcohol (Daeppen et al., 2014; Kim, K e Kim, J., 2015; Valentin et al., 2014), cocaine (Díaz-Morán et al., 2015), tobacco (Marques e Arandas, 2011; Kushkestani et al., 2020) and crack (Narvaez et al., 2015) dependents.
Chemical dependents in treatment at health institutions were also observed and the literature evidenced low scores, which indicates a deterioration of the QoL of these individuals at the beginning of treatment (Lopes et al., 2014; Marcon et al., 2014; Narvaez et al., 2015; Oliveira et al., 2014). However, it was also observed that significant improvements in the perception of QoL might occur not only during the interventions but also at the end of treatment (Daeppen et al., 2014; Morgan et al., 2003; Oliveira et al., 2006).
Thus, by understanding the QoL perception of patients with chemical dependence or drug users, together with their possible determinants, it is possible to guide, improve and adapt public policies for the implementation of a more suitable treatment aimed at enhancing health (Marini et al., 2013).
Materials and Methods
Study design and Participants:
This is a quantitative-descriptive and cross-sectional study. A total of 52 patients participated in this study, of which 47 were men and 5 were women. These patients were admitted to treatment at Ismael Abdel Aziz Rehabilitation Center for Chemical Dependency (CRDQ) in the city of Manaus, Brazil. We excluded from the study patients who had cognitive impairment, were underage and those who had not complete the three months referring to the treatment period in the institution.
CRDQ receives people for treatment of chemical dependency.For this, the multiprofessional team works in several areas, such as: cognitive-behavioral psychotherapy, occupational therapy, art therapy, physical training, physical therapy and cognitive stimulation with reading and logic games.Each of these activities lasted 60 to 90 minutes and was offered once a week, in addition to psychoeducational workshops and psychological support group sessions.
We observed a prevalence of men (M=90.45), aging between 18 and 27 years (M=50%), single (M=65.4%), with complete secondary education (M=34.6%) and family income of up to 4 minimum wages (M=40.4%). Patients reported using oxi as a dependence drug (M=25%), followed by cocaine (M=19.25), being consumed every day (M=53.8%) for at least two years. They also reported having relatives who use drugs (M=65.4%), with the siblings being the most cited (M=32.4%).
Questionnaire of socio-demographic data and about drug use:
A socio-demographic questionnaire was elaborated according to the literature. It is composed of closed questions about personal data, questions about frequency and use of substances, form of access to drugs, substance that caused dependence and family history of drug use (Capistrano et al., 2013; Ortega-Pérez et al., 2011; Peixoto et al., 2010).
Medical Outcomes Study 36–Item Short-Form Health Survey:
The SF-36 is a generic instrument for easy comprehension and rapid application to assess the perception of QoL. Its applicability is independent of gender, age or disease. The instrument is divided into eight concepts: physical functioning, physical role functioning, bodily pain, general health, vitality, social role functioning, emotional role functioning and mental health. For each question, there is only one response. At the end, the scores are decoded and evaluated according to the score obtained, being 0 the minimum score and 100 the maximum, indicating the worst and the best QoL, respectively (Oliveira et al., 2014; Paes et al., 2012).
This study was performed in a rehabilitation center, where treatment is offered through a 3-month hospitalization. This place was chosen for convenience, as it is the only public institution in this model in the city. This research was approved by the Ethics Committee under the CAEE number 50909215.8.0000.5020.
After individually explaining the aims of the study, the patients who agreed to participate signed the Term of Free and Clarified Consent (TFCC). Psychologists and psychology undergraduate students collected data during a 5-month period. The socio-demographic questionnaire and the SF-36 were applied individually at the beginning (first month) and the end of the treatment (third month); the SF-36 was reapplied to the same patients in private rooms at the research site.
Data Analysis:
Data were analyzed by Excel 2010 program (Microsoft Office Enterprise) and Statistic Package for the Social Sciences (SPSS), version 17.0. The descriptive analysis contemplated: frequencies, means, percentages and standard deviation of the sample. A significance level of (p < 0.001) was adopted for the SF-36 variables. The effect size analysis between the comparisons of the SF-36 concepts was performed through Cohen’s d.
Results and Discussion
In the first application of SF-36 during the first month of treatment, the assessment of the QoL identified low scores in all 8 concepts of the instrument, as well as in the physical and mental components. The results can be observed in Table 1 below. Although there is no consensus cohort note in the literature on the SF-36 scale, it can be inferred that 0 and 100 are respectively the worst and the best QoL. Values above 70 points should indicate a good or preserved QoL (Vanelli e Freitas, 2011).
According to Martins et al. (2012), the initial assessment of the QoL reflects the actual general health situation of the drug user upon arrival at the health institute, as well as the harm caused by substance abuse. Oliveira et al. (2014) and Campêlo et al. (2017) mention that heavy drug abuse or chemical dependence leads to carelessness on the part of the user with their mental and physical health, which culminates in a progressive degradation of the body, mental and social life. Hence, reflecting in the low scores found for QoL.
Studies with substance users obtaining similar results have been reported in the literature. For instance, a research conducted in North Carolina with 619 participants found that drug addicts had worse QoL scores in all concepts (physical functioning, M= 8.9; physical role functioning, M=62.6; bodily pain, M=56.7; general health, M=57.6; vitality, M=50.7; social role functioning, M=58.4; emotional role functioning, M=60.8 and mental health, M=46) when compared to the general population (Costenbader et al., 2007).
Similarly, Narvaez et al. (2015) observed low QoL in cocaine users, especially in the following concepts: physical functioning (M=69); general health (M=66); emotional role functioning (M=68); mental health (M=66) and bodily pain (M=65). Morgan et al. (2003) corroborated with these data when they reported low scores for QoL in some concepts, for instance: general health (M=66), vitality (M=54), social role functioning (M=69), emotional role functioning (M=62) and mental health (M=59).
The low scores of drug users in QoL may be associated with the type of drug used by them, for example, in the case of cocaine and its derivatives physical damage to the internal organs is accentuated, which may lead to persistent discomforts and severe health problems. However, the type of substance used is apparently not the only factor capable of causing a low QoL. The drug use intensity, the emotional and social relationships of the individual, in addition to the previous history of health (physical and mental) can influence the way in which he or she perceives his or her QoL (Campêlo et al., 2017; Costenbader et al., 2007; Narvaez et al., 2015).
Marcon et al. (2014) findings, when studying the correlation between QoL and depression, corroborate with this understanding. According to the authors, all SF-36 concepts were affected, with emphasis on mental health = 60 and vitality = 66. Díaz-Morán et al. (2015) observed that cocaine users and with psychiatric comorbidity had worse QoL in all concepts, mainly on emotional role functioning = 47, mental health = 49, vitality = 49, social role functioning =58, bodily pain = 63 and general health =63, when compared to dependents without comorbidities. Benaiges et al. (2012) observed that when comparing groups of chemical dependents with and without psychiatry comorbidities, the former had worse QoL in the following concepts: emotional role functioning = 46, vitality = 42, mental health =50, general health = 50 and social role functioning = 60.
Comparatively, the results found in the literature approximate to the findings of this research (with respect to the first application), observed by the following concepts (Table 1): physical functioning (M=69) and (DP=18,05), physical role functioning (M=44) and (DP=33,5), bodily pain (M= 62) and (DP=20,8), general health (M=65) and (DP=21,3), vitality (M=58) and (DP=20,04), social role functioning (M= 54) and (DP=20,3), emotional role functioning (M= 30) and (DP=33,3) and mental health (M=52) and (DP=18,5). It is worth noting that, although only QoL was evaluated in this study and, therefore, there is no data regarding the presence or absence of comorbidities, along with their severity, the means found in the 8 SF-36 concepts are similar to those abovementioned studies. Hence, these results indicate that the patients interviewed had QoL as compromised as drug users who also have psychiatric comorbidities.
Lev-Ran et al. (2012) reported that, among marijuana users, women had worse QoL in the mental component (M=42) and the following concepts: vitality = 48, social role functioning = 44, emotional role functioning = 43 and mental health =42, when compared to men. Menezes (2006) identified low scores in women in the concepts: bodily pain (M=47), vitality (M=40) and mental health (M=33). These results are consistent with a study by Domingo-Salvany et al. (2010), in which the worst QoL on general health (M=35.9) was observed in women when compared to men. In our research, the assessment of gender and QoL (the first and the second application, referring to the first and third month of treatment) showed no statistically significant difference. This fact may be explained due to the reduced number of women admitted for treatment who participated in the study, making it difficult to evaluate and correlate QoL and gender.
The low QoL in women may also be due to the fact that they are more concerned with physical health, complain more, consume more medications and also show more feelings; unlike men who tend to have a less serious attitude towards diseases and less frequently seek treatments for illnesses (Benincasa, 2010; Kim, K. e Kim, J., 2015; Moreira et al., 2013). Comparatively the results diverge from this research, which found a greater quantitative of men (M=90.4%) hospitalized for treatment.
With regard to the level of chemical dependency and QoL, Menezes (2006) found that moderate and severe users had worse QoL in all concepts: physical functioning (M=71 and 63), physical role functioning (M=18 and 16), bodily pain (M=56 and 52), general health (M=42 and 43), vitality (M=43 and 9.1), social role functioning (M=32 and 29), emotional role functioning (M=54 and 22) and mental health (M=32 and 11), respectively. Comparably, Benincasa (2010) observed low scored of QoL in subjects that were frequent and heavy users, with emphasis to the concepts: vitality (M=41), mental health (M=38), physical role functioning (M=68), bodily pain (M=53), general health (M=50), social role functioning (M=52) and emotional role functioning (M=41). These findings from the literature validate our results since 53.8% of the sample reported using drugs daily, and 88.5% reported using it for more than 2 years. Therefore, the low QoL of the interviewees verifies the existence of a relationship between frequency and time of use.
Moreira et al. (2013) found even worse QoL among drug users who had less than 8 years of study in life, in the physical (M=14.8), psychological (M=13.90), social (M=13.4) and environment (M=12.9) concepts, when compared to those with a higher level of education. In agreement, Faker (2009) identified a statistically significant association between low or no education and the concepts of bodily pain (M=53.4), social role functioning (M=59.2) and mental health (M=62.4). Likewise, we observed statistically significant differences in the results of our research in the second application of SF-36 in the concept of bodily pain (M=40), with higher scores for high school graduates. Besides, marginally significant differences in the vitality concept were observed, with those being high school graduates (M=34) and incomplete higher education (M=32.3) having the highest scores.
It was noted, in the present research, that those with a higher level of education (complete high school - 34.6%) had better performance in the bodily pain and vitality concept, compared with those with the lowest level of education (incomplete elementary school - 32.7%) obtained the worse performance in the mentioned concepts. Faker (2009) explained that eventually, the lower the level of schooling, the more difficult it becomes for the subject to obtain adequate information or even understand instructions and/or explanations on various factors, including health care and treatment, in addition to information on drugs and their effects.
On the other hand, the best score for vitality (presence or level of energy and/or fatigue) of subjects with higher levels of education seems to indicate that not only the understanding of information is necessary for QoL but also for procedures and interventions. Also associated with this, the individual with a better understanding of their health and treatment apparently have more resources concerning the motivation for treatment and change. In the stages of action and maintenance of the transtheoretical model of change, it is important to have the energy to perform and maintain consistent changes in their behavior towards health.
In the present study, the results indicated that all SF-36 concepts showed statistically significant differences (p<0.001) between the applications (first and second). Thus, when comparing the results of the two applications, it is evident that the values of the averages increased, indicating an improvement in the QoL of the participants in all concepts.
Similar results were obtained by Lahmek et al. (2009), who reported that, after 3 weeks of hospitalization, patients had a significant improvement in QoL values, with final concept averages close to 50 (value for the French population): mental health (M=48), emotional role functioning (M=46), social role functioning (M=47), vitality (M=51), general health (M=48), bodily pain (M=49), physical role functioning (M=47) and physical functioning (M=49). Similarly, Morgan et al. (2003) noticed, when comparing the beginning and the end of the treatment (3 months) through SF-36, a significant improve among all concepts, with emphasis to mental health (M=59 to M=72), social role functioning (M=68 to M= 84) and emotional role functioning (M=62 to M=80).
Lahmek et al. (2009), Daeppen et al. (2014), Gonçalves et al. (2020) and Barati et al. (2021) comment that positive results regarding QoL improvement may be influenced by several factors, for example: not using the substance at the time of treatment, resocialization through meetings and groups, therapeutic environment, harm reduction programs of substance, self-image improvement, self-esteem and self-care, and psychosocial support.
We also observed that, when comparing the results obtained between the two applications of the SF-36, and analyzing the effect size from Cohen's d, the largest score differences that occurred in specific concepts were in physical functioning, which increased to (M= 95.3) and in vitality (M=86.8). Similar data were obtained by the study of Marcon et al. (2014), in which, among all concept, physical functioning (M=86.4) and vitality (M=66.1) presented better scores, indicating good QoL in the physical component. Comparably, Oliveira et al. (2014) found good QoL scores in the concepts physical functioning (M=72.1) and vitality (M = 62.6).
The improvement in the QoL of these two concepts indicates that the physical damage caused by drug consumption has been attenuated, possibly due to the treatment, allowing a significant increase in QoL perception. It is thus perceived the importance of the treatment with a focus in the most diverse areas of the subject, be it physical, emotional and social. It should be noted that, as in the studies above, the patients in this sample were also being treated and similarly to what happens in CAPS ad, the CRDQ also opts to use both the abstinence and the harm reduction aspects. Therefore, although the patients were in treatment aiming not necessarily abstinence, the therapy used helped to improve their QoL (Marcon et al., 2014).
In this study, low QoL was identified in all 8 concepts at the beginning of treatment of chemical dependent patients, which suggests that abusive drug consumption undoubtedly affects not only health but also other areas of life of the patients. At the end of the treatment, the QoL showed significant improvements, which may indicate that the therapy used and adherence to the treatment enhanced the various concepts of QoL evaluated. However, only two concepts showed greater statistical differences, which imply the need to observe the other concepts and establish strategies so that they may also, through therapeutic interventions, undergo positive changes that are identified through higher scores.
It is also suggested that future research should investigate concepts not evaluated in this study, for instance, environmental and spiritual. The literature has demonstrated the importance not only of the physical, social and family environment where the subject is inserted but also of the presence or not of religious practice, as risk factors or protection to the use of drugs. Also, the period of evaluation of the QoL could be extended to more than 3 months, aiming to know the extent of the impact of the therapeutic interventions beyond the treatment period. An expanded sample is also suggested in the sense of greater representativeness between men and women, providing also the possibility for a broader knowledge about the phenomenon studied.
Funding: Not applicable for that section
Conflicts of interest/Competing interests: The authors declare no conflict of interest.
Code availability: Not applicable for that section
Ethics approval: The authors declare this research was approved by the Ethics Committee under the CAEE number 50909215.8.0000.5020
Consent to participate: The authors declare that all patients who agreed to participate signed the Term of Free and Clarified Consent
Consent for publication: The authors approved the version to be published and agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. Also Nazaré Hayasida made substantial contributions to the conception, design and interpretation of data of the work and Raquel Lira made substantial contributions for the acquisition, analysis and interpretation of data.
Authors would like to acknowledge all the staffs of Ismael Abdel Aziz Rehabilitation Center for Chemical Dependency (CRDQ) and all involved patients in this research.
Authors also acknowledge Amazon Federal University (UFAM) for all support and FAPEAM - Research Support Foundation in Amazonas.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
